Surrogates, not sight
Today's endpoints infer tissue effect from electrical and mechanical proxies. The lesion is never observed, only estimated.
RFA & PFA • REAL-TIME LESION ASSESSMENT
Recurrence is the main unsolved problem in atrial fibrillation ablation. AblaView®* is a catheter delivering either RFA or PFA energy that provides real-time lesion assessment (contact, stability, lesion size, durability of the ablations, gap detection, pop prediction). The system's ability to detect during ablation whether the procedure will be ineffective was confirmed at 100% specificity for durable PFA at three-month follow-up in the first-in-human study, peer-reviewed in Europace.
*The device presented is under preclinical/clinical investigation. It is not FDA approved nor CE labelled.
Recurrence is the main unsolved problem in atrial fibrillation ablation. The physician creates lesions in an atrial wall that is typically 0.6 mm to 1 mm thick, guided by surrogates: contact force, power, time, impedance. None of them show the lesion itself, so gaps are found months later, when the arrhythmia returns.
Today's endpoints infer tissue effect from electrical and mechanical proxies. The lesion is never observed, only estimated.
Non-durable lesions and gaps in the ablation line reveal themselves after the procedure, driving redo interventions.
At under a millimeter of atrial wall, the margin between an incomplete lesion and a perforation is small. Resolution matters.
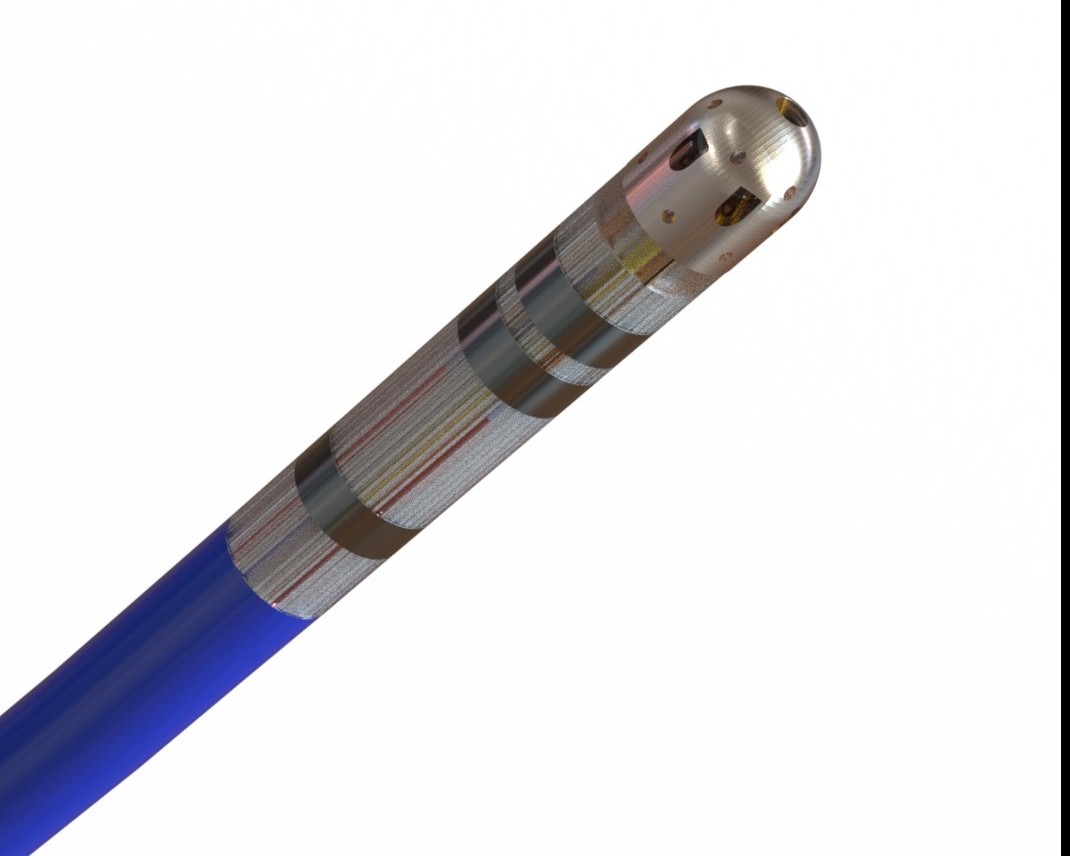
Polarization-Sensitive Optical Coherence Reflectometry measures tissue birefringence directly, with 50µm axial resolution. Intracardiac ultrasound is around 200µm, so PS-OCR is 4 to 5 times higher resolution. This margin matters because atrial walls are thin, typically 0.6 mm to 1 mm thick, and susceptible to perforation. A 1310 nm swept-source laser resolves individual tissue layers at the catheter tip. The physics is what makes the unique performance of AblaView® possible.
Realtime. Direct. No surrogates. The lesion durability and gap detection in realtime are the largest unsolved problem in EP ablation procedures. AblaView® is the only platform that closes it.
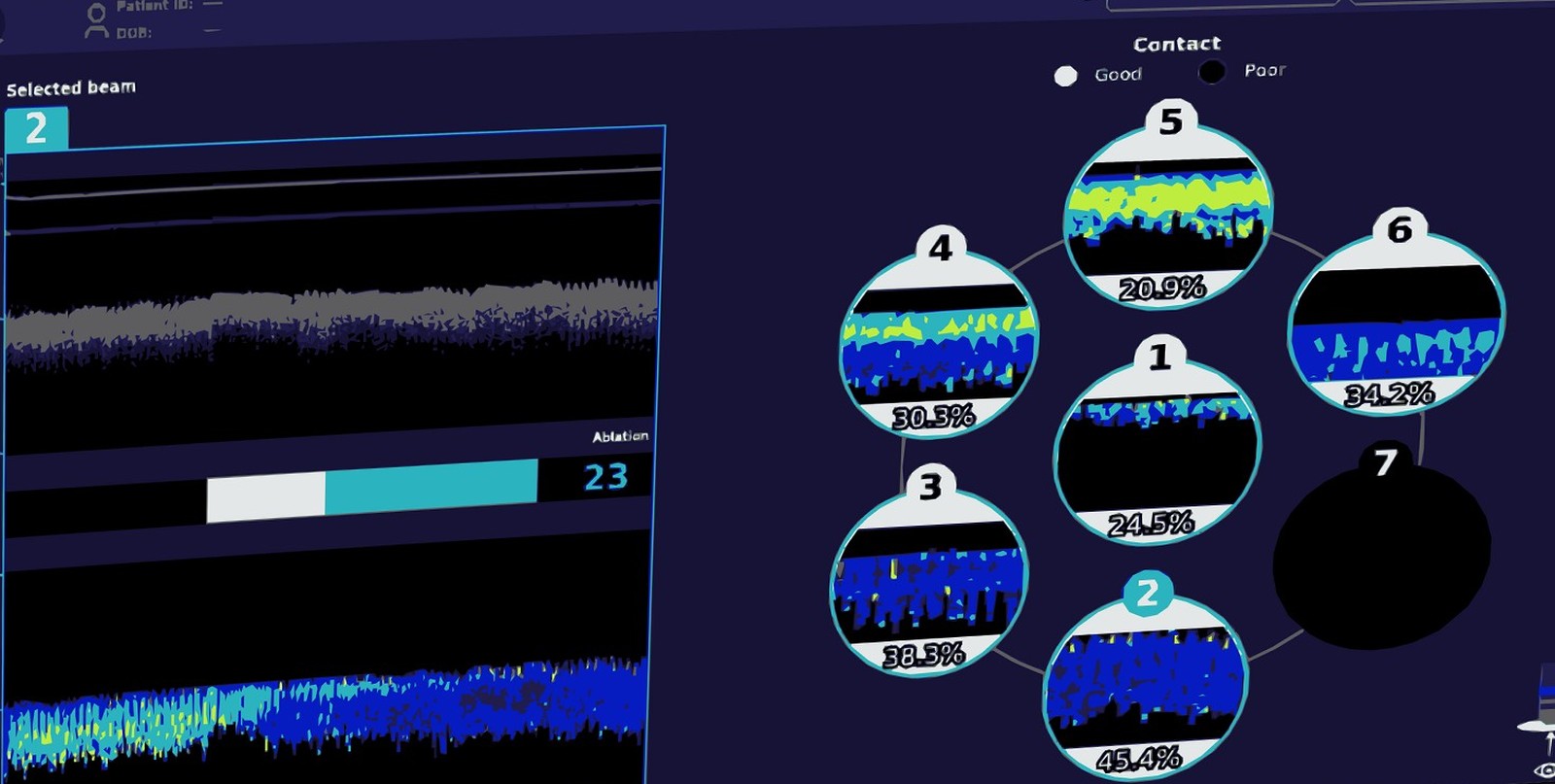
Contact quality, stability & catheter orientation. Direct optical assessment of contact quality, stability, and catheter orientation at the tip. Real-time identification of gaps during the procedure.
Lesion size (diameter and depth) · pop prediction. Optical readout of lesion diameter and depth during RF delivery, plus a validated steam-pop risk model, both measured directly from birefringence at the catheter tip.
Durability prediction. 100% specificity for durable PFA at three-month follow-up in the first-in-human study (n=10, no hemolysis, no neurovascular complications). Peer-reviewed in Europace, February 2025.
Published in Europace, 2025. Preclinical PS-OCR validation in Circulation, 2024.
Co-author on the AblaView® first-in-human Europace publication, February 2025. Proctor during the first-in-human cases.
Co-author on the AblaView® first-in-human Europace publication, February 2025. Proctor during the first-in-human cases.
Lead author on the AblaView® PS-OCR preclinical study published in Circulation, 2024. Directs the Preclinical Cardiovascular Lab at Sunnybrook. Specialist in preclinical evaluation of novel ablation devices.
The team, the platform, and the dual-energy catheter, told by the people building it.
ABLAVIEW CORPORATE FILM. 2:59. DEVICE SHOWN IS INVESTIGATIONAL.
70+ patents covering polarization-sensitive optical tissue imaging and optical-guided ablation. 9 jurisdictions. Owned outright. No licensing obligations to any third party.
Every AblaView® procedure produces optical tissue measurements, and the preclinical program pairs them with histological ground truth: 860+ ablations to date. This paired corpus trains the AblaView® Clinical AI Engine that runs the live display, and it grows with every case. Good correlation has been observed between the animal and human PS-OCR output.
Dive deeper into the science and the data behind AblaView®.