50µm
Axial resolution. 4 to 5× higher than intracardiac ultrasound. Critical because atrial walls are typically 0.6 mm to 1 mm thick and susceptible to perforation.
Polarization-Sensitive Optical Coherence Reflectometry (PS-OCR) measures tissue birefringence directly with 50µm axial resolution, 4 to 5× finer than intracardiac ultrasound. The physics is what makes the unique performance of AblaView® possible.
The device presented is under preclinical/clinical investigation. It is not FDA approved nor CE labelled.
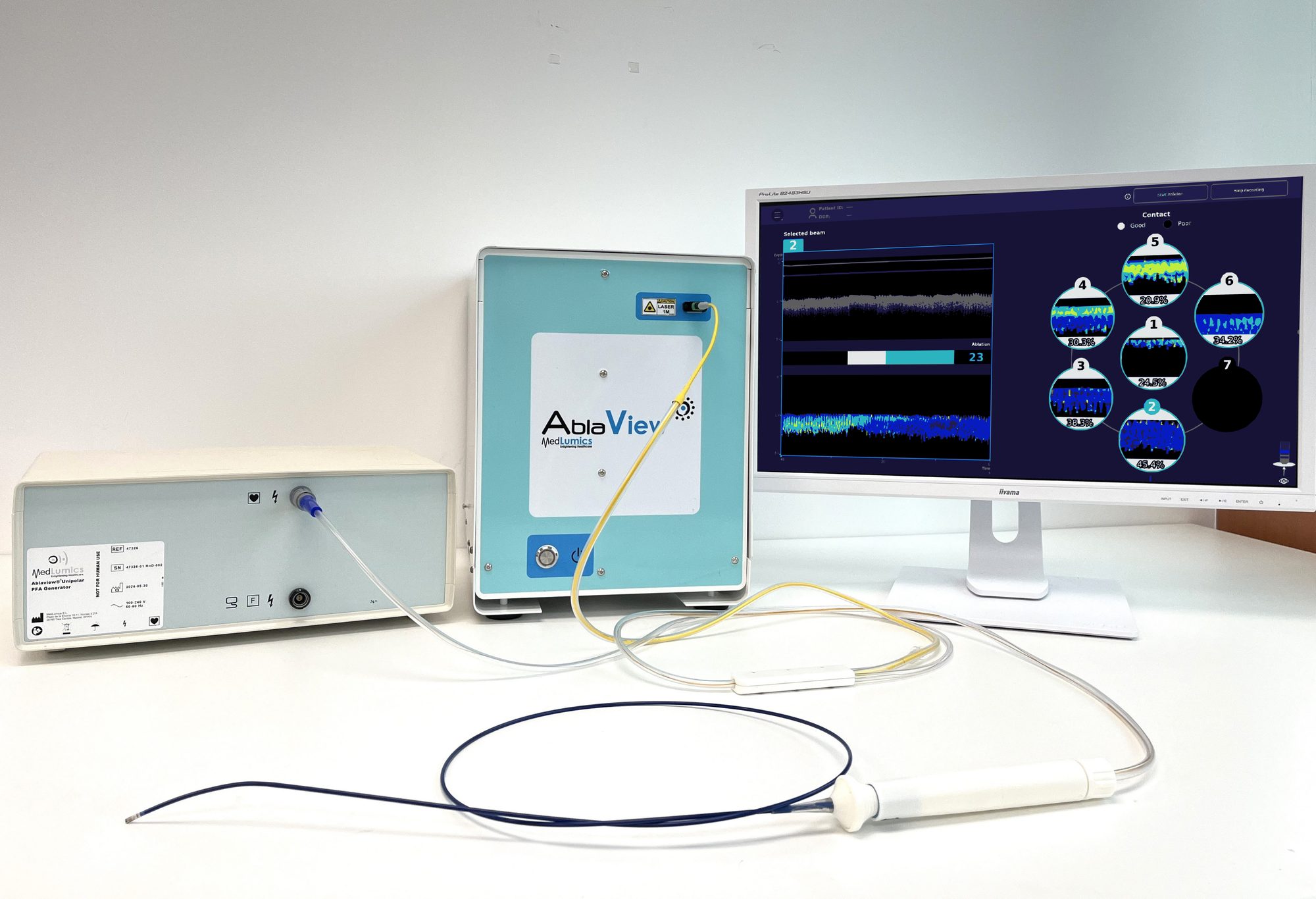
Standard mapping systems rely on indirect markers that do not assess energy absorption in the tissue. AblaView® is uniquely providing direct mapping of tissue structure and organisation, by analysing the polarisation state of backscattered light at the catheter tip with a 1310 nm swept-source optical sensor.
Axial resolution. 4 to 5× higher than intracardiac ultrasound. Critical because atrial walls are typically 0.6 mm to 1 mm thick and susceptible to perforation.
Many things no one else can do simultaneously, in real time and without surrogates. Organised by what is common to both energy modalities and what is specific to RF or PF.
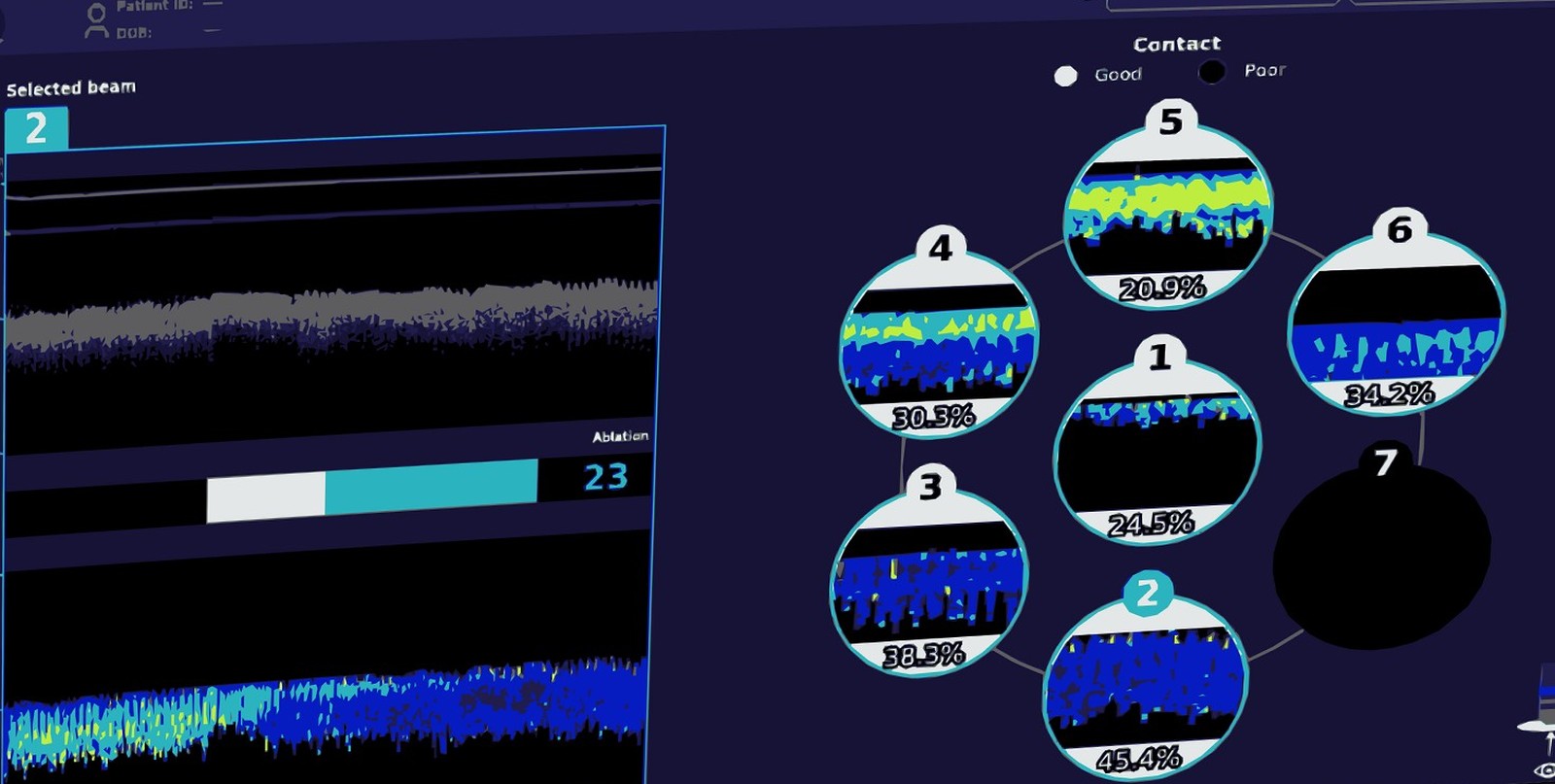
Direct optical assessment of contact quality, contact stability and catheter tip orientation. Independent of force sensors and impedance.
Direct mapping of tissue structure and organisation at the catheter tip from the birefringence signal.
Preserved tissue between lesions is the precursor to reconnections. AblaView® identifies it during the procedure.
Optical readout of lesion size during RF delivery, measured directly from birefringence at the catheter tip.
Validated model for steam-pop risk based on the temporal evolution of the birefringence signal.
Optical readout is immune to PFA-induced cellular stunning. 100% specificity for durable PFA at three-month follow-up in the first-in-human study (Europace, 2025).
Hardware, data and IP, each built over years, none easily replicated.
Optical sensor, console and catheter integration developed over twelve years of catheter-focused R&D. AblaView owns the working system outright.
Pre-clinical 22.4 TB and clinical 2.69 TB (Y14 + Y06), paired with histology. Built across twelve years of catheter-focused work.
9 jurisdictions. Owned outright. No licensing obligations to any third party.
Detailed catheter dimensions, generator outputs and channel-level specifications are shared with qualified partners under NDA, and full disclosure follows regulatory approval. The summary below is the public, system-level view.
| Specification | Value |
|---|---|
| Imaging Modality | PS-OCR (Polarization-Sensitive Optical Coherence Reflectometry) |
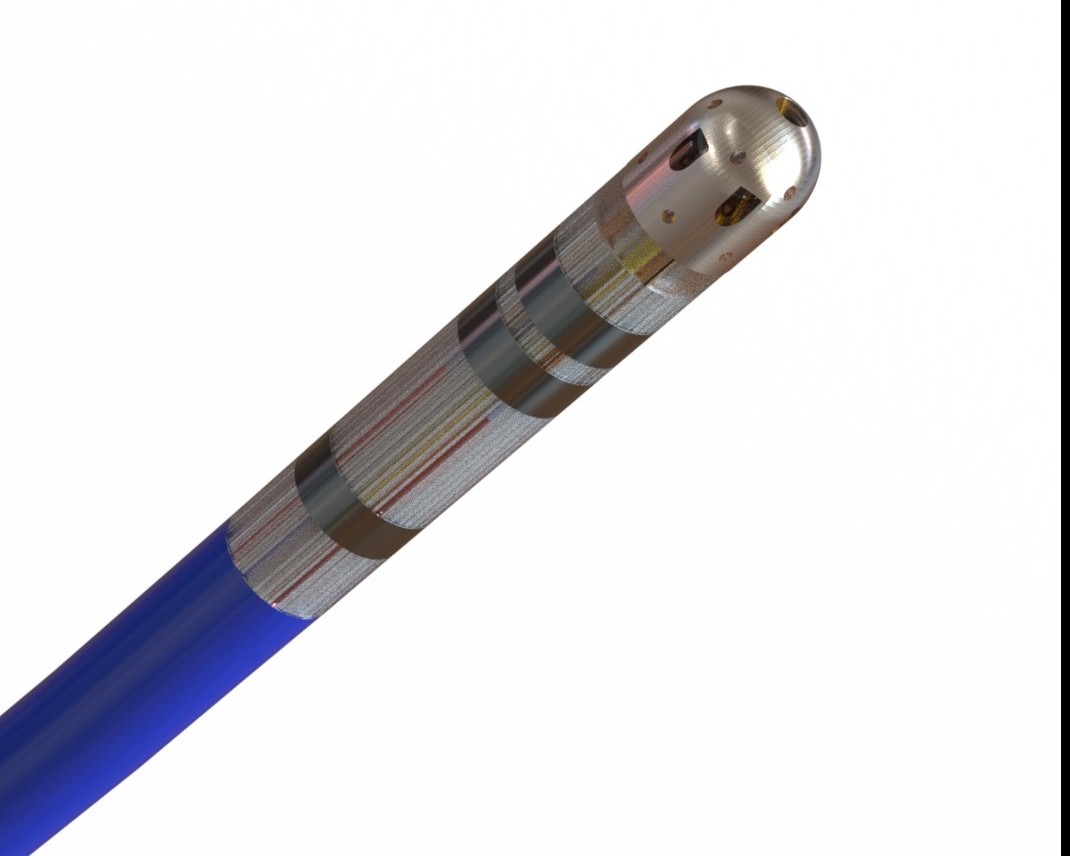
| Optical Sensor | 1310 nm swept-source. Eight parallel channels at the catheter tip (seven PS-OCR measurements plus one reference channel). |
| Axial Resolution | 50µm. Roughly 4 to 5× finer than intracardiac ultrasound. |
| Clinical Refresh Rate | 50 ms GUI refresh (20 fps), including acquisition and AI inference. |
| Energy Modalities | RF and PFA in a single catheter. Modality-agnostic optical guidance. |
| AI Processing | Clinical AI Engine on NVIDIA IGX Orin with deterministic inference. |
The Clinical AI Engine turns the PS-OCR optical signal into clinical indicators in real time. The public summary is below. Full Software-as-a-Medical-Device classification, training dataset, validation protocol and change-control plan are shared with qualified partners under NDA.
| Module | Function |
|---|---|
| M1. Tissue Classification & Gap Detection | Identifies tissue type at the catheter tip from the optical return signal and detects preserved tissue between lesions during the procedure. |
| M2. Contact Assessment | Quantifies catheter-to-tissue contact quality and stability in real time from the optical signal, with catheter tip orientation. |
| M3. Lesion Prediction | Uses birefringence loss as the optical marker of irreversible tissue change. Indicates durable lesion formation during PFA and lesion size during RF. |
| M4. Safety Detection | Independent CPU-based safety boundary layer. Runs in parallel with the AI stack and is not dependent on it. |
PS-OCR is a fibre-based optical sensing modality that measures the birefringence of tissue, the optical property that arises from organised fibrous structures such as collagen and aligned myocardium. In cardiac muscle, ablation disrupts the underlying tissue organisation and changes its birefringence signature in a way that can be measured optically in real time, at the catheter tip, with 50 micron axial resolution, roughly 4 to 5 times finer than intracardiac ultrasound.
The Clinical AI Engine is a four-module software system that turns the PS-OCR optical signal into clinical indicators in real time. Module M1 performs tissue classification and gap detection (collagen, fat, nerve, vessel, conduction system). Module M2 assesses catheter-tissue contact and stability. Module M3 predicts lesion size and durability. Module M4 is an independent CPU-based safety layer that detects steam-pop risk, microvascular obstruction risk, and proximity to critical structures.
Sub-50 ms end-to-end. The signal chain runs on NVIDIA IGX Orin with TensorRT FP16 inference and deterministic scheduling, which is fast enough to support closed-loop safety decisions during active ablation delivery.
Yes. The catheter supports both radiofrequency (RF) and pulsed-field ablation (PFA) in a single device. The optical guidance layer is modality-agnostic and is designed to integrate with third-party ablation platforms across energy modalities.
More than 25 terabytes of proprietary PS-OCR data accumulated across twelve years of catheter-focused bench, preclinical, and first-in-human work, paired with histology. Preclinical data accounts for the majority of volume; clinical (Y14 and Y06 datasets) contributes approximately 2.7 terabytes. The full dataset was acquired outright by AblaView in 2026 and is owned with no licensing obligations.
The system is investigational and not FDA approved. The current working assumption is a 510(k) pathway with predicate analysis underway, supported by a Predetermined Change Control Plan drafted against FDA 2024 final guidance. Timelines depend on FDA pre-submission outcomes and are not committed publicly.
AblaView® can be deployed as an optical-only evaluation layer, as a full optical evaluation plus ablation system, or as an SDK / OEM integration. The catheter is always paired with the AblaView console because the optical connection and ablation interface are co-engineered.
AblaView® catheter + AblaView® console (with the Clinical AI Engine). Used alongside the partner’s existing mapping and generator stack to add real-time optical lesion assessment to the procedure.
Single-vendor stack delivering RF or PFA energy with integrated PS-OCR guidance end-to-end.
AI Engine outputs streamed into a partner’s UI as a licensed overlay. Deepest integration; requires bilateral engineering and regulatory alignment.
Medical-device partnerships are long-cycle. Partnership conversations benefit from early architectural alignment. Interface contracts are shared under mutual NDA so engineering teams can validate fit before terms.